InfoShop
Contents
Welcome to InfoShop. A website about political systems such as anarchy, political history and political news. Here you can learn more about different political systems, their benefits and drawbacks.
Political Systems
It is very important to understand how different political systems work if you want to be able to understand and improve the world around you. We therefore feature in depth articles about different political systems and how they work.
 Anarchism is a political philosophy and movement that rejects involuntary, coercive forms of hierarchy and is sceptical of authority.The philosophy of anarchism, and the movements that have sprung from it, are diverse and they embody many (sometimes conflicting) attitudes, tendencies and schools of thoughts. Historically and contemporary, the various branches of anarchism have complex relationships with ideologies such as communism, collectivism, libertarianism, and trade unionism. Phenomena such as civilization, religion, and technology are lauded in some anarchist movements and sharply criticized or outright rejected in others. Read our in depth Anarchy FAQ:
Anarchism is a political philosophy and movement that rejects involuntary, coercive forms of hierarchy and is sceptical of authority.The philosophy of anarchism, and the movements that have sprung from it, are diverse and they embody many (sometimes conflicting) attitudes, tendencies and schools of thoughts. Historically and contemporary, the various branches of anarchism have complex relationships with ideologies such as communism, collectivism, libertarianism, and trade unionism. Phenomena such as civilization, religion, and technology are lauded in some anarchist movements and sharply criticized or outright rejected in others. Read our in depth Anarchy FAQ:


Famous historical figures
Below you will find information on important historical political figures. Individuals that have had a large effect on the history and development on modern politics.
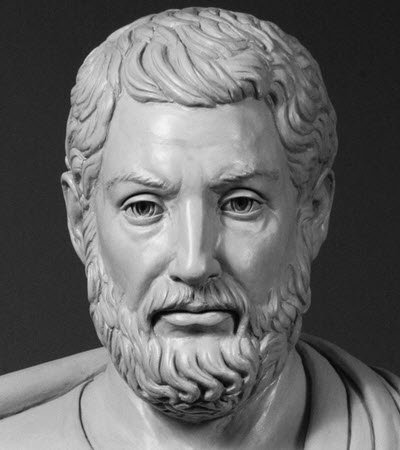
Cleisthenes ( Κλεισθένης), also known as Clisthenes, was an Athenian lawgiver in ancient Greece. He is credit with reforming the constitution of ancient Athens in 508 B.C. to promote democracy, and is therefore known as the father of Athenian democracy. Read more…
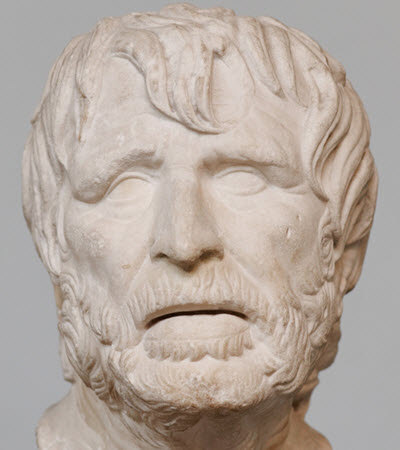
Ephialtes was a politician in ancient Athens and an early leader of Athens democratic movement. In the late 460s BC, he oversaw reforms that decreased the power of the Athenian governing council Areopagus. Read more…

Pericles ( Περικλῆς) was an influential politician and general during the Golden Age of Athens. He lived from circa 495 to 429 BC, and his most powerful period was between the Greco-Persian Wars and the Peloponnesian War. Read more…
Featured historical articles
Below you will find articles about historical events. You can find a lot more articles about historical events by browsing our website. The articles below are simple a small sample of our articles that we have chosen to feature. We regularly change the articles that we feature here.

Read our article about how the Athenian revolution helped created the foundation for the modern democracy. Read article.
The capitalistic financial system
In this section of the site you can read articles about how to financial system of the world really works. You can read about how the rich use the system to make themself richer, how the system exploits people and how it can lift people out of poverty as well as about how you can use cryptocurrency and other types of trading to improve your own financial situation.
Capitalism is a dual edge sword and it is very important to know about both its benefits and its drawback. That is to only way to be able to use the system to improve the world.

Cryptocurrencies is an economical revolution that takes the power from the banks and make it easier for private individuals to make secure private transactions. Read more…

The foreign exchange market (Forex market) is a market where different FIAT currencies are traded against each other. The market set exchange rates around the world. Read more about online FOREX trading.

CFD certificates are advanced financial instruments that allow day traders to make highly leverage trades and make large profits from small market movements. Read more about online CFD trading and CFD platforms.

The finance market is filled with scams and fake gurus. People who prey on the dreams of other people and steal their money. Read more…